Peyronie’s Disease Treatment
Scroll down to view operative videos and figures depicting several Peyronie’s disease procedures.
Injections for Peyronie’s Disease
If one does feel that their Peyronie’s disease is disallowing sex, then Dr. Engel’s first line therapy before surgery is contemplated is injection therapy.
If one does feel that Peyronie’s disease is disallowing sex, then Dr. Engel’s first line of therapy before surgery is contemplated injection therapy.
If one feels that their Peyronie’s disease is disallowing sex, then our first line of therapy before surgery is contemplated is injection therapy, whereby the Peyronie’s plaque is injected over a series of several injections with a substance designed to either melt the scar directly (Xiaflex) or indirectly (Verapamil). There have been several injections used for Peyronie’s, including interferon and steroids, but Xiaflex and Verapamil are the most studied and have the best data. If a patient is contemplating injection therapy, they will typically return for a second consultation with Dr. Engel with a photo demonstrating their erect penis and its maximal curvature or defect. Typically, Dr. Engel uses Verapamil after extensively using Xiaflex upon its initial release. For Xiaflex, there are strict rules to allow for insurance coverage, including stability for a year and greater than 30-degree curvature, and the cost can be significant for those with high deductibles. Also, it is a small-volume injection, and Dr. Engel prefers a higher-volume injection to treat the entire plaque. However, ultimately, the choice of injection is up to the patient, of course. Over time, though, Dr. Engel more and more frequently is going back to Verapamil over Xiaflex due to its simplicity, low cost, and apparent lower risk profile. A final consideration is that for Xiaflex to get its FDA approval, it was forced to warn patients against sexual activity for almost the entire duration of treatment, and the patient must be made aware of possible penile fractures.
With both substances, patients will be asked to perform a traction protocol designed to stretch the scar as it softens from injections. Verapamil is administered over 12 office visits, each two weeks apart, with an evaluation after the sixth injection as to whether one notices improvement that would justify the second round of six injections. Xiaflex is also given over 24 weeks but in four cycles of three visits spanning a week at a time. Xiaflex is FDA-approved, and Verapamil is not, but both yield similar results – approximately 50% of patients will notice a statistically significant reduction of their curvature (although not necessarily clinically significant), and over 80% will notice a reduction of discomfort. It is unclear if the excellent pain reduction is simply due to the passage of time or not, as typically, the pain will resolve spontaneously over time, even without injections. Injections will be less effective for constrictions or hinging and ineffective if the plaque is fully calcified. Xiaflex is extremely expensive, although it is often covered by insurance. Verapamil is a very inexpensive, generic medication. Neither injection medication precludes surgery if ineffective.
Surgical Treatment of Peyronie’s Disease
If injection therapy fails, and the patient still feels as if, without further treatment, fulfilling sexual function will simply not be possible, then surgical treatment can be offered. It should be stressed that sometimes a patient may do honest soul-searching and simply admit that the curvature gets in the way of his psychological health. At times, this alone, if well expressed and/or if injections fail, may justify a simple procedure such as plication (see below).
For those patients with little to no erectile dysfunction with stable disease and possible failure of other treatments, then either a plication procedure or an incision and grafting procedure is offered, with the latter offered only in the most severe curvature cases. Before offering an incision and grafting, excellent penile blood flow and, thus, erections must be documented by an ultrasound penile blood flow study to limit the risk of post-operative erectile dysfunction.
If a patient has severe erectile dysfunction such that he relies on injections or a vacuum pump for erections, this would be the time to strongly consider penile prosthesis placement. The prosthesis is an excellent way to address both the problems of severe ED and penile curvature. Often the combination of just the prosthesis and manual manipulation called modeling will straighten the penis. If more is needed, either plication or, now, more commonly, incision and grafting while the prosthesis is in place is highly effective.
Procedures that remove the plaque are generally no longer performed as they produce unacceptable rates of impotence. Surgery for Peyronie’s disease should generally be considered a last resort. See below for examples of each procedure.
Plication Procedure
A plication procedure is an outpatient surgical procedure where the fixation of the plaque is counteracted by permanent sutures placed in the penis opposite the plaque. In essence, it creates a second fixation point, much like what can be seen with The Leaning Tower of Pisa in Italy. This is a relatively simple operation, with less than a 1% chance of impotence after the surgery and little chance of numbness. However, the major problem with this operation is that it will shorten the penis, and the shortening is very much related to the degree of curvature. A perfect curvature for a plication would be approximately 30 degrees, as in such cases, shortening is not at all severe and is usually very well tolerated by the patient.
In some cases, patients still prefer plication over more involved, riskier operations and will simply accept shortening as a tradeoff. Dr. Engel has found that as long as a patient is informed and makes the choice himself, patients still end up very happy with a straight but somewhat shorter penis. If Peyronie’s surgery were purely about straightening the penis, then almost all would accept shortening. But it is also typically about psychology, and thus, some patients, already struggling with the situation, find this new impairment to any degree unacceptable.
Learn more about Penile Plication for Peyronie’s Treatment (graphic content) >>
Incision & Grafting Procedure
An incision and grafting procedure for Peyronie’s disease is a complex reconstructive procedure that Dr. Engel performs as a last resort for severe Peyronie’s disease. Such a procedure is reserved for patients with severe curvature that has not responded to injection therapy. Usually, a round of injection therapy is tried first to see if the curvature can be lessened, at least to the point where plication might be offered. Patients who opt for this surgery usually have good to excellent erections before surgery, as patients with co-occurring severe erectile dysfunction are typically managed with a penile prosthesis and possible Peyronie’s procedure.
Patients must understand that incision and grafting carries with it a 3-5% chance of impotence, as well as a 5-7% chance of some degree of permanent penile numbness. This procedure leads to more post-operative discomfort than a plication procedure. But, in this procedure, the plaque is lengthened, and the penis is restored to nearly its original erectile length. Most patients find that this benefit outweighs the higher risk and recovery, and most, when given the choice, choose grafting over plication as it seems like a perfect solution. However, long-term results amongst surgeons who offer this operation have shown a large incidence of long-term graft contraction such that the results are not as good as seen in the first year.
For this reason, Dr. Engel recommends plication unless severe curvature is present. The right patient for this procedure is a patient whose penis is bent to the degree that they are already sexually inactive, often with their partner complaining of pain. Such patients feel that they have little to lose by proceeding as something must be done lest they give up on sexual activity altogether.
The incision and grafting procedure is performed in a hospital setting, but patients are usually sent home the same day with a compressive dressing and office follow-up the next day. The sensation of the penis is checked the day after surgery, and patients are asked to come to the office in two weeks. At that time, erections with pills like Viagra are encouraged, as is gentle traction to keep the graft from contracting. Complete recovery may take one to two months.
Warning, the video below represents an actual procedure – The content is graphic
Peyronie’s Surgery Combined With Penile Prosthesis Surgery
As mentioned above, in patients with severe erectile dysfunction where erection is perhaps achieved by injection therapy or, more rare, a vacuum erection device, certainly one could consider penile straightening and then continue with injections or a vacuum device for ED. However, most patients see the logic in placing a penile prosthesis as they will be having penile surgery already, and this seems to solve all the problems at once. Sometimes, insurance considerations exist where the prosthesis is not covered for the indication of ED but is covered if Peyronie’s disease is also considered. Penile prosthesis placement is covered extensively elsewhere on the site, but below are two examples of Peyronie’s cases where a prosthesis has also been placed. It should be noted that the first thing that is tried to correct curvature is a series of bending maneuvers on the penis with the prosthesis inflated called “modeling.” However, this usually has limited success and does have some risk of urethral injury. It is crucial to discuss the patient’s desires before surgery with regards to how straight a penis he needs to be happy so that the least intervention can be applied to get there.
Figure 1: Photos before (a) and after (b) a prosthesis has been placed in a patient with severe ED and classic Peyronie’s upward curvature. Modeling has failed, and straightening has been achieved with plication sutures. Note the continued presence of mild curvature, as usually perfect straightness is not sought to limit shortening.

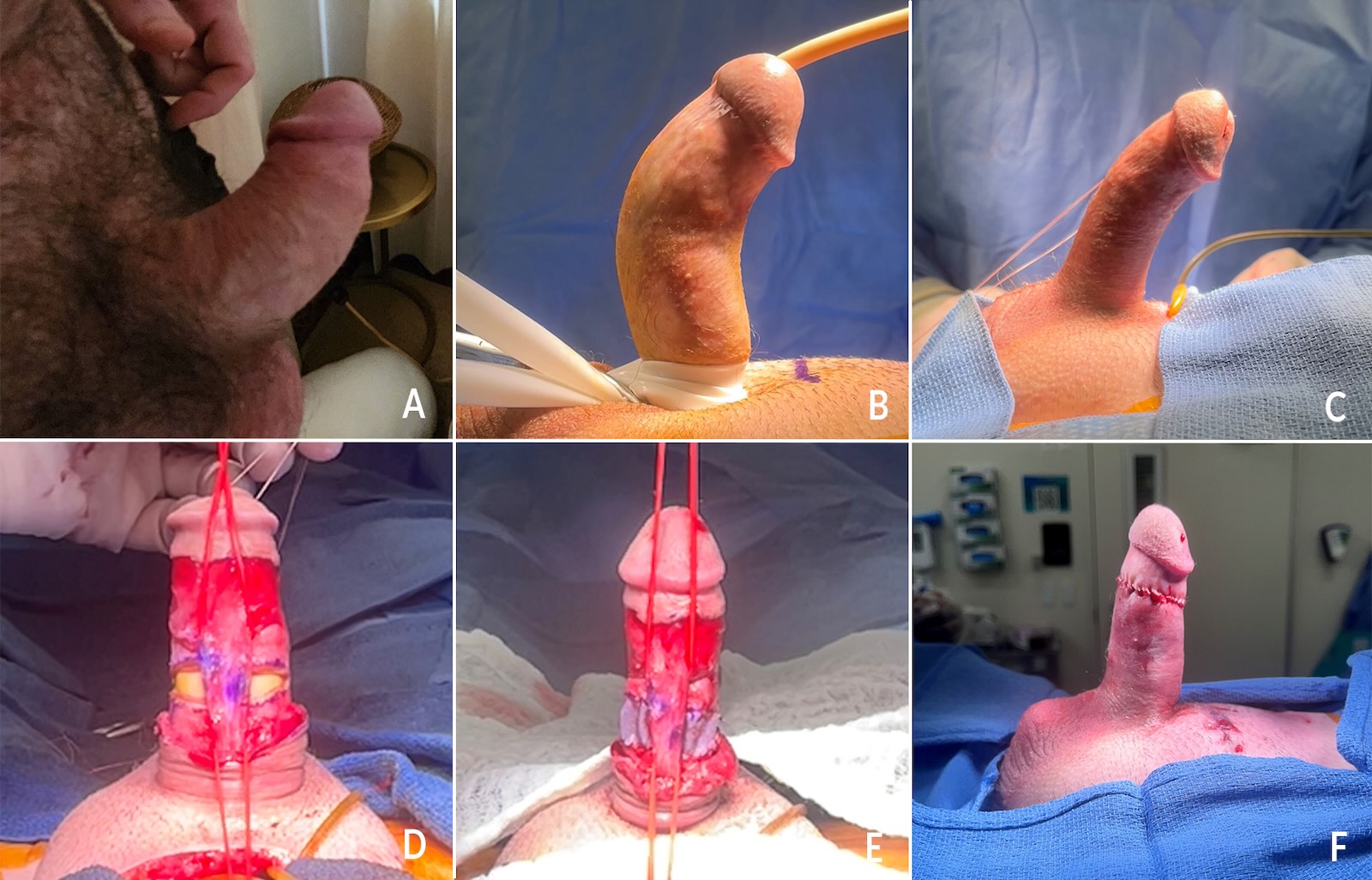
Figure 2: Photos showing a typical photo brought to Dr. Engel by the patient, followed by all steps of prosthesis placement with incision and grafting. (a): self-taken photo by the patient (is “Peyronie’s selfie”.) (b): artificial erection in the OR (is “prosthesis grafting before”) (c) appearance after failed modeling and prosthesis inflated (is “prosthesis grafting still bent”) (d) incision has been made in plaque exposing prosthesis cylinders, note sensory nerves dissected and raised (is “prosthesis grafting release”) (e) graft sewn in place into defect made by incision, note crinkly to allow for expansion (is “prosthesis grafting graft”) (f) penis now perfectly straight upon prosthesis inflation (is “prosthesis grafting straight”).